

- Sie haben noch keine Artikel in Ihrem Warenkorb.
Winter Coronavirus (COVID-19) Infection Study: estimates of epidemiological characteristics, 21 December 2023 (Nachrichten)
This publication describes the prevalence of the SARS-CoV-2 virus in England and Scotland. SARS-CoV-2 is a coronavirus that causes COVID-19.
Test positivity describes the proportion of lateral flow device (LFD) tests taken by participants in the study that are positive for SARS-CoV-2. However, because tests are imperfect, some tests will return false negative results when an infected individual is tested. A very small number of positive tests may also be false positives when an uninfected individual is tested.
Prevalence is an estimate of the proportion of the population who are infected. It is calculated by adjusting positivity to account for imperfect test performance. This correction is important in this study as LFD tests are used. LFD tests return more false negatives than the polymerase chain reaction (PCR) tests that were used in the previous Office for National Statistics (ONS) Coronavirus (COVID-19) Infection Survey (CIS). Estimates of prevalence are useful for individuals who want to understand their risk of exposure to SARS-CoV-2.
To ensure estimates are representative of the wider population, the prevalence estimates from this cohort are adjusted through reweighting. The reweighting approach used by this study aims to provide an estimate of prevalence that is representative of the whole population in terms of age, geography, and sex. The study only includes participants aged over 2 years and therefore all the analyses conducted, and population projections used in this report do not include individuals aged under 3 years.
In future publications we will include estimates for incidence, the number of new infections each day; and the infection hospitalisation risk, the probability that someone infected with SARS-CoV-2 will require hospital admission. Information on unweighted positivity is available from the ONS Winter CIS publication.
Main points
There has been an increase in prevalence of SARS-CoV-2 in England and Scotland during the 2 weeks leading up to 13 December 2023.
In England and Scotland, the estimated prevalence of SARS-CoV-2 on 13 December 2023 was 4.2% (95% Credible intervals (CrI): 3.3%, 5.4%), which is equivalent to around 2,549,000 individuals (95% CrI: 1,996,000 to 3,236,000) being infected with SARS-CoV-2. This corresponds to around 1 in 24 people (95% CrI: 1 in 30 to 1 in 19).
In England, the estimated prevalence of SARS-CoV-2 on 13 December 2023 was 4.3% (95% CrI: 3.3%, 5.4%), which is equivalent to 2,333,000 individuals (95% CrI: 1,825,000 to 2,953,000) being infected with SARS-CoV-2. This corresponds to around 1 in 24 people (95% CrI: 1 in 30 to 1 in 19).
In Scotland, the estimated prevalence of SARS-CoV-2 on 13 December 2023 was 4.1% (95% CrI: 3.0%, 5.6%), which is equivalent to 215,000 individuals (95% CrI: 160,000 to 293,000) being infected with SARS-CoV-2. This corresponds to around 1 in 24 people (95% CrI: 1 in 33 to 1 in 18).
On 13 December 2023 it was estimated that prevalence was higher for individuals aged between 18 to 44 years than for those aged over 65 years. Prevalence was estimated to have increased across all age groups in the 2 weeks up to 13 December 2023.
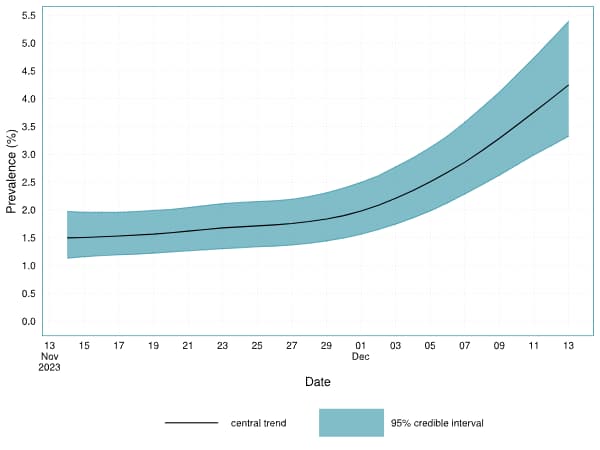
Figure 1. Estimates of prevalence over time in combined England and Scotland between 14 November 2023 and 13 December 2023

Estimated prevalance in England and Scotland
On 13 December 2023, the estimated prevalence of SARS-CoV-2 in England and Scotland was 4.2% (95% CrI: 3.3%, 5.4%). Prevalence has increased in the past 2 weeks from 1.8% (95% CrI 1.4%, 2.3%) on the 29 November 2023 (Figure 1 and Table 1).
On 13 December 2023, prevalence of SARS-CoV-2 was estimated to be 4.3% (95% CrI: 3.3%, 5.4%) in England and 4.1% (95% CrI: 3.0%, 5.6%) in Scotland. The estimated prevalence in England and Scotland have risen in the past 2 weeks from 1.8% (95% CrI: 1.4%, 2.3%) and 1.8% (95% CrI: 1.3%, 2.3%), respectively (Figure 2a and 2b).
Figure 2a. Estimates of prevalence over time in England between 14 November 2023 and 13 December 2023

Figure 2b. Estimates of prevalence over time in Scotland between 14 November 2023 and 13 December 2023

Table 1. Current estimates of prevalence in England and Scotland, and separate estimates for England and Scotland
| Date | Location | Prevalence |
|---|---|---|
| 13 December 2023 | England and Scotland | 4.2% (95% CrI: 3.3%, 5.4%) |
| 13 December 2023 | England | 4.3% (95% CrI: 3.3%, 5.4%) |
| 13 December 2023 | Scotland | 4.1% (95% CrI: 3.0%, 5.6%) |
Estimated prevalence in England and Scotland by age
The estimated prevalence for the age groups in England and Scotland from the 14 November to 13 December 2023 is referred to in Figure 4 and Table 3. Prevalence was estimated to be higher for individuals aged between 18 to 44 years compared to those aged 65 years and over. Prevalence has notably increased across all age groups in the past 2 weeks, particularly in young adults (Figure 3 and Table 2). As the sample sizes used to estimate prevalence for each age group are smaller than the overall study’s sample size, there is higher uncertainty compared to national estimates, which is reflected in wider credible intervals.
Figure 3. Estimates of prevalence over time by age group in combined England and Scotland between 14 November 2023 and 13 December 2023

Table 2. Combined England and Scotland current estimates for prevalence by age group
| Date | Age group | Prevalence |
|---|---|---|
| 13 December 2023 | 3 to 17 years | 3.2% (95% CrI: 2.1%, 4.8%) |
| 13 December 2023 | 18 to 34 years | 5.8% (95% CrI: 4.1%, 8.0%) |
| 13 December 2023 | 35 to 44 years | 5.7% (95% CrI: 4.4%, 7.5%) |
| 13 December 2023 | 45 to 54 years | 4.6% (95% CrI: 3.6%, 5.9%) |
| 13 December 2023 | 55 to 64 years | 4.0% (95% CrI: 3.1%, 5.1%) |
| 13 December 2023 | 65 to 74 years | 2.6% (95% CrI: 2.0%, 3.3%) |
| 13 December 2023 | 75 years and over | 2.0% (95% CrI: 1.4%, 2.6%) |
Estimated prevalence in the regions of England
The estimated prevalence for the regions of England from the 14 November to 13 December 2023 is referred to in Figure 4 and Table 3. The prevalence has increased in every English region over the past 2 weeks and in particular London and the South East. There is considerable uncertainty in the estimated prevalence for the regions of England. As the sample sizes used to estimate prevalence for each region of England are smaller than the overall study’s sample size, there is higher uncertainty compared to national estimates, which is reflected in wider credible intervals.
Figure 4: Estimates of prevalence over time in regions of England between 14 November 2023 and 13 December 2023

Table 3. Current estimates of prevalence in the regions of England
| Date | Region | Prevalence |
|---|---|---|
| 13 December 2023 | North East | 3.6% (95% CrI: 2.5%, 5.1%) |
| 13 December 2023 | North West | 3.8% (95% CrI: 2.7%, 5.1%) |
| 13 December 2023 | Yorkshire and Humber | 3.4% (95% CrI: 2.4%, 4.6%) |
| 13 December 2023 | East Midlands | 3.4% (95% CrI: 2.3%, 4.6%) |
| 13 December 2023 | West Midlands | 3.4% (95% CrI: 2.5%, 4.7%) |
| 13 December 2023 | East of England | 4.4% (95% CrI: 3.3%, 5.9%) |
| 13 December 2023 | London | 6.1% (95% CrI: 4.6%, 8.1%) |
| 13 December 2023 | South East | 4.8% (95% CrI: 3.6%, 6.3%) |
| 13 December 2023 | South West | 3.7% (95% CrI: 2.7%, 5.0%) |
Methodology
Demographics are over or underrepresented in the study, and it is important to adjust for this to produce nationally representative estimates of SARS-CoV-2 prevalence.
A Multilevel Regression and Post-Stratification (MRP) approach is used to estimate the prevalence for different subgroups. MRP helps reduce the uncertainty in prevalence estimates for subgroups that might be under-represented or under-sampled in the original study, offering a more representative and accurate estimation of prevalence for the entire population. This is achieved by incorporating external information about the size of different subgroups. The MRP model used estimates a national prevalence trend over time, and adjustments are then made to this national trend for each combination of age group, sex, and region. The difference between prevalence in different subgroups may vary over time, and this model is able to make different adjustments at different points in time. All the analyses conducted in this report do not include individuals aged under 3 years.
An important part of understanding prevalence is adjusting for imperfect test sensitivity, which causes false negatives to be observed in the data. False negatives are when an individual is truly positive, but their test provides a negative result. We developed a model that estimates how many false negatives we expect to observe in the data, allowing us to adjust for the presence of false negatives when calculating prevalence. The model also adjusts for test specificity, though with high test specificity it has a minimal influence on the estimated prevalence.
In the survey, once a participant tests positive for SARS-CoV-2, they are asked to take repeat tests every other day until they return 2 negative tests. This repeat testing data is used to estimate the false negative rates of LFDs, over time, for the cohort. This allows us to further model the test sensitivity as it evolves over the epidemic phases. As the study gathers further data the diagnostic performance of the LFD test will be updated.
Individuals appear to be more likely to test earlier or before the testing window if they are symptomatic. As a result, tests taken earlier in the window are more likely to be positive than tests taken later in the testing window. This model includes an adjustment for this effect, based upon which day of their testing window they took their test.
Data sources
Based on responses from the Winter Coronavirus (COVID-19) Infection Study (Winter CIS), commissioned and funded by UK Health Security Agency (UKHSA), to deliver real-time information to help assess the effects of COVID-19 on the lives of individuals and the community, and help understand the potential winter pressures on our health services. The study has been launched jointly by ONS and UKHSA, with data collected via online questionnaire completion and self-reported lateral flow device (LFD) results from previous participants of the COVID-19 Infection Survey (CIS). The ONS 2023 to 2024 population projections will be published alongside the report on positivity.
Authors
Alex Glaser – UKHSA
Alexander Phillips – UKHSA, University of Liverpool
Andre Charlett – UKHSA
Christopher Overton – UKHSA, University of Liverpool
Jonathon Mellor – UKHSA
Julie Day – UKHSA
Martyn Fyles – UKHSA
Owen Jones – UKHSA
Robert Paton – UKHSA
Steven Riley – UKHSA, Imperial College London
Thomas Ward – UKHSA
Glossary
Prevalence
The estimated proportion of individuals who are infected with the SARS-CoV-2 virus at a given point in time.
Incidence
The estimated number of new infections occurring on a given day.
Infection hospitalisation risk (IHR)
Measures the risk of hospital admission given that you have been infected with the SARS-CoV-2 virus.
Infection fatality risk (IFR)
Measures the risk of death given that you have been infected with the SARS-CoV-2 virus.
Vaccine effectiveness
How effectively vaccinations protect people from health outcomes such as infection, symptomatic disease, hospitalisation, and mortality.
Quelle: gov.uk
Den ersten Kommentar schreiben.
Antworten
Sie müssen eingeloggt sein, um einen Kommentar zu schreiben.