

- Sie haben noch keine Artikel in Ihrem Warenkorb.
Masks Work. Distorting Science to Dispute the Evidence Doesn’t (Nachrichten)
New mask studies relying on a medical paradigm do not erase decades of engineering and occupational science that show they work
Masks work. Especially respirator-style N95 masks.
Amid an ongoing pandemic and outbreaks of influenza and RSV caused by airborne viruses, arguing over the virus-blocking power of masks remains one of the COVID era’s signature follies. Disconcertingly, despite decades of evidence of their efficacy, some of the disagreement comes from a few in the medical field itself, misusing science and endangering lives.
Most recently a Cochrane review, which systematically assesses multiple randomized controlled trials, provoked headlines after claiming a lack of evidence that masks prevent transmission of many respiratory viruses. Not for the public, health care workers, or anyone. “There is just no evidence that they make any difference,” the lead author said in a media interview. This brought an unusual chastisement from the Cochrane Library’s editor-in-chief, who stated it was “not an accurate representation of what the review found.”
That wasn’t the first time something like this has happened. Late last year, a randomized controlled trial claimed that N95 respirators were no better than medical (or surgical) masks for health care workers. Whereas scientists, engineers and occupational health and safety experts highlighted flaws (see its comments section) in the study, these two episodes point to a bigger fundamental question: whether these types of trials are suitable to test how well physical interventions like masks reduce viral transmission.
Medical assertions of exclusive “ownership” over the science of masks when they are used during a pandemic ignore the fact that they represent a well-understood engineered solution, with decades of widespread and successful use behind them. Demands to reject this evidence reflect a failure to recognize and respect interdisciplinary expertise that has undercut the global pandemic response.
Placing randomized trials above other types of research such as observational, lab and modeling studies, has interfered with the COVID response. A randomized trial approach that allows a few studies to cancel out a huge body of research from other disciplines has no basis in science.
Enthroning these trials atop medical decision-making started with the best of intentions. In the 1980s, experts wanted to better integrate scientific knowledge into medicine. Decisions then varied widely among practitioners based on disparate reading, experience and education. Refining medical decision-making to make it more repeatable, consistent and linked to evidence marked the laudable birth of the evidence-based medicine movement.
This effort included establishing a “hierarchy of evidence,” the idea that some types of evidence are more useful to medical decision-makers than others. Expert opinion and observational studies are at the bottom of the pyramid, randomized trials in the middle, and at the top, systematic reviews of these trials, where researchers compile and review several clinical trial results to make broader, more conclusive statements as happens with Cochrane review.
Randomized trials underlie much of medical research, because the human body is messy. A chemical effective in a lab or an animal model might turn out useless, or even harmful, once inside a human body—or only in some people, depending on genetics, environment or underlying illness. Randomizing trial participants averages out that noise and reduces biases. By comparing treatment outcomes between randomly selected groups, we can hope to isolate effects, making these trials a “gold standard” in medical research. However, they often take time, many participants (especially if the expected differences are small) and big budgets. Even the most rigorous of trials can’t tell you if a treatment would have been effective with a different protocol. For example, a trial of seat belts in airplane crashes couldn’t say they work in cars.
Because these trials are so narrowly focused—and can disagree—systematic compilations and reviews such as those produced by the Cochrane organization can make medical decision-making quicker and easier. Relying on such reviews, of course, trades convenience over the rigor of digesting each study and gaining real knowledge; this is one concern with them.
For masks, are randomized trials an appropriate way of evaluating a basic engineered safety system in the first place? We don’t rely on such trials for seat belts, bike helmets or life jackets, and the oft-cited randomized trial of parachutes is an old running joke. Why is that so hilarious? What do the engineers know that doctors don’t?
In many scientific disciplines randomized trial methods are fundamentally inappropriate—akin to using a scalpel to mow a lawn. If something can be directly measured or accurately and precisely modeled, there is no need for complex, inefficient trials that put participants at risk. Engineering, perhaps the most “real-world” of disciplines, doesn’t conduct randomized trials. Its necessary knowledge is well-understood. Everything from highways to ventilation systems—everything that moves us, cleans our air and our water, and puts satellites into orbit—succeeds without needing them. This includes many medical devices. When failures like a plane crash or catastrophic bridge collapse do occur, they are recognized and systematically analyzed to ensure they don’t happen again. The contrast with the lack of attention paid to public health failures in this pandemic is stark.
“Does a mask protect me from aerosolized virus?” or “Does this seat belt keep me from flying through the window in an accident?” are different types of questions than “Does aspirin reduce death rates after a heart attack?” Imprisoning engineering and the natural sciences at the very bottom of an evidence hierarchy—at the same level as an expert opinion—is a mistake. As with seat belts, whether people use masks properly matters, but no randomized trial could conclude seat belts “don’t work.” At best, that type of trial would be a truly inefficient way to assess specific instructions and incentives to get people to use them properly.
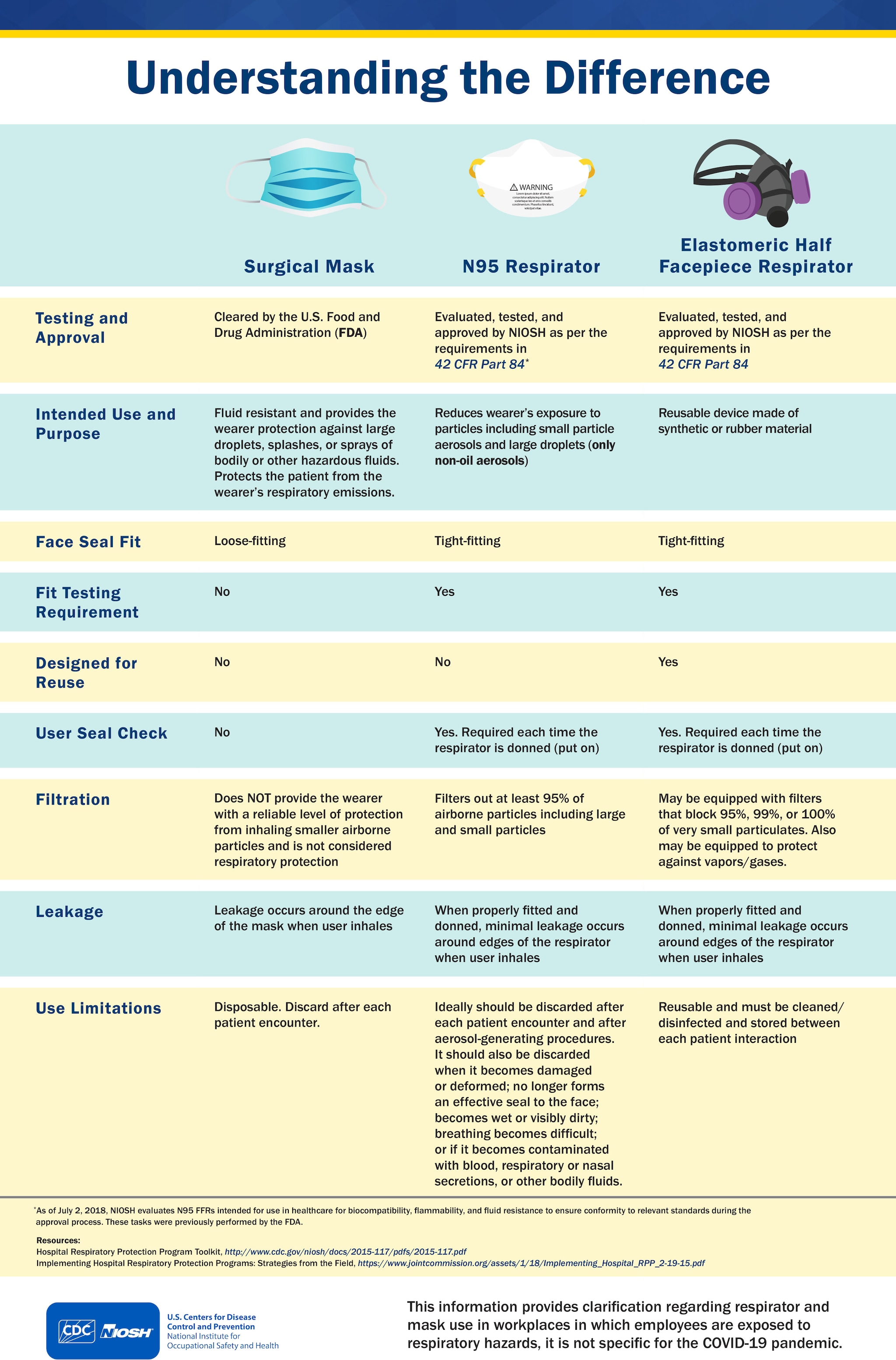
A well-understood technology, respiratory protection has been validated over decades, with standards (NIOSH in the U.S., CSA in Canada) that codify protection from viruses and bacteria. Mining, biomedical research, chemical processing, pharmaceutical production and many more industries follow these laws and standards worldwide. Without exaggeration, millions of people trust their lives to the effective “real-world” science of respirators, with no need for randomized trial evidence.
{kind=link}
It is therefore deeply concerning that prominent medical figures have misrepresented the protection provided by masks, when the evidence supports N95 respirators or better, ideally with two-way masking.
Medical policy makers failed to learn the lesson of the 2003 SARS-1 outbreak, exposed again in the current global pandemic: a novel pathogen requires a precautionary approach that includes airborne respiratory protections until proven otherwise. With millions dead and immense—and still growing—personal and economic damage inflicted by long COVID, failing to adjust now will continue to do enormous harm.
It is not too late to do better.
This is an opinion and analysis article, and the views expressed by the author or authors are not necessarily those of Scientific American.
Quelle: scientificamerican
Den ersten Kommentar schreiben.
Antworten
Sie müssen eingeloggt sein, um einen Kommentar zu schreiben.